
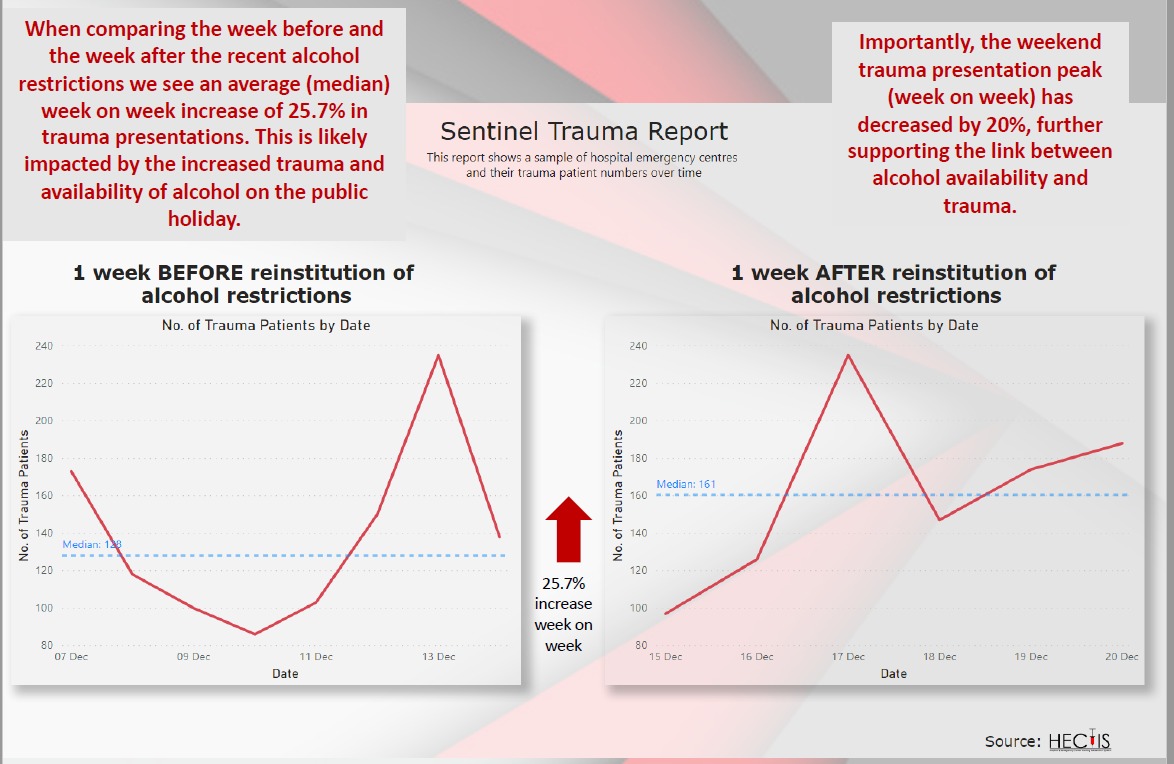
At a recent digicom hosted by Alan Winde, the Western Cape premier made it patently clear that trauma presentations were rising rapidly: by 26% across the five hospitals in the Western Cape sentinel trauma surveillance system, even after restrictions on gathering numbers and on alcohol sales, and a tightened curfew from 16 December.
Christmas comes but once a year. Yet every year, like this repeated refrain, doctors and nurses brace themselves for the post-Christmas fallout as our festivities drag well into the New Year. Casualties of knife lacerations, gunshot wounds, road traffic collisions and gender-based violence, all present to hospital, each one requiring assessment, management, very often admission, and sometimes ventilation in ICU.
This year is no different.
And yet it is also completely different. We are standing on the sidelines witnessing two epidemics collide as our hospitals fall over the brink to cope with patients ill with Covid-19 and those with conditions related to alcohol.
Both conditions are preventable.
Most will have heard and read of the tumult in Western Cape hospitals and many will have experienced it first-hand. Western Cape Covid-19 case numbers followed the increases in the Garden Route and Eastern Cape earlier in December. Patients have waited in line for beds, for oxygen, for nurses; ambulances have driven from hospital to hospital following divert announcements; staff are sick with Covid-19, others are in quarantine, many are exhausted; oxygen capacity is on red alert; and politicians have stated the severity of the situation.
Requests have gone out for medical and nursing volunteers to assist to tide over the next few days, and some will answer the call. But there will not be enough.
We are not prepared for what awaits over New Year.
We were prepared for the first Covid-19 wave, with the heavy-handed lockdown intended to ensure hospital capacity would be available. It was. The merits of the lockdown and its disastrous effects on the broader economy, and the inaccuracies of the projections from modelling continue to be important to debate and learn from, but right now, we need to identify key drivers of the soaring admissions and act on these.
Now, not after the crisis.

We present two targeted interventions for government consideration, both based on sound evidence, to implement immediately to cover the period up to 3 January 2021. We have seen that when the will is there, the government has been able to move with alacrity.
It should do so again.
Interventions needed to curb alcohol-related admissions
Alcohol use, and especially heavy drinking, is causally related to trauma admissions. This relationship is undisputed by scientists worldwide. Availability, price and affordability of alcohol, as well as marketing practices have increasingly been shown to impact on drinking and associated harms.
At a recent digicom hosted by Alan Winde, the Western Cape premier made it patently clear that trauma presentations were rising rapidly: by 26% across the five hospitals in the Western Cape sentinel trauma surveillance system, even after restrictions on gathering numbers and on alcohol sales, and a tightened curfew from 16 December (read the Western Cape statement here and watch it on FB here).
Upwards of 30% of patients presenting to trauma require admission.
By taking action to reduce trauma presentations across these five and other hospitals, it should be possible to reduce the demand for beds in general wards, theatre time, ICU beds, ventilators and on hospital staff and materials.
In a previous Daily Maverick article (Charting a healthier way forward for alcohol in South Africa, now and into the future, 27/7/20), one of the authors (Charles Parry) proposed a 10-point plan for better managing alcohol-related harm and to reduce pressure on hospital staff and other resources when the second alcohol sales ban was lifted.
Only one of those measures is currently in place: the restriction of sales of liquor for off-site consumption between 10am and 6pm, from Mondays to Thursdays. This should remain in place as further reducing hours and days of sale may have the unintended consequence of crowding stores and driving panic-buying.
Many of the other evidence-based approaches to reducing alcohol-related harms require major policy shifts and community consultation, but we need to implement further interventions fast. Additional considerations, which can be rapidly enacted, would be to suspend all on-premise sales of alcohol until the 3 January 2021 and to ban special-price promotions on alcohol at this time. The latter will send a clear message to the industry and the public that marketing of cheap alcohol during a pandemic is not ethical.
Recommendation 1: Maintain current restrictions on off-consumption liquor sales and suspend all on-premise sales and consumption of alcohol e.g. in bars, restaurants and taverns; and prohibit discounted alcohol promotions in all media and in liquor outlets
Interventions to curb Covid-19 transmissions
SARS-CoV-2 (the virus that causes Covid-19) is transmitted by droplets from the nose, mouth or eyes passing from one person to another. It is increasingly recognised as also spread via the airborne route.
Regardless of route of transmission, we increase our risk
of acquiring Covid-19 when we come closely together in confined and crowded spaces. The definition of a close contact, according to the National Institute of Communicable Disease, is being within 1 metre of someone with confirmed Covid-19 (whether symptomatic or not) for 15 minutes or more, without a mask. It is not a long time, especially when you are having fun, and masks only provide protection when used in combination with other measures.
Add alcohol to that mix, and we begin to predictably lose our inhibitions. We forget to wash our hands, move closer towards our family member or friend, pull off our uncomfortable mask, and stay longer than we intended.
Our current regulations limit indoor gatherings to 100 people and less than 50% capacity in any establishment. This remains reasonable for the longer term, and the onus to manage this is appropriately placed on restaurants, businesses and places of worship. We understand the need to balance economic imperatives with health and safety measures. Restaurants are in their busy season and reducing capacity further will undermine their sustainability and profit margins. Additional restrictions should therefore focus first on alcohol restrictions as outlined above, but consideration should be given to further reducing the number of people permitted to gather indoors to 50. Until 3 January 2021.
In the meantime, meeting outdoors in small groups is much safer for all, limiting this to usual household members and close friends only.
Recommendation 2: Further reduce indoor gatherings to 50 people and maintain less than 50% capacity in indoor venues
Both the above recommendations are intended as short-term interventions only and attempt to balance the needs of the economy and the desires of the public with the urgent need to reduce hospital presentations.
We note them to be blunt tools, and potentially regressive, impacting the poor worse than the rich. We note the many upstream social determinants of alcohol use and abuse in our country. We note the evidence-based interventions to reduce alcohol-related harms outlined by the World Health Organisation and ourselves, including restricting on- and off-premise outlet density; increased price and taxation, including minimum unit pricing; and restricting alcohol advertising. These all remain critical to the broader public health discussions around alcohol which we must have as a country once the worst is over.
Right now, we need to act and we urge the government to consider our recommendations. We commit to collection and collation of trauma and admission data towards the end of January to provide an indication of the utility of such actions and to build the evidence base lest we find ourselves in this situation again in December 2021. DM/MC
By Nandi Siegfried & Charles Parry
Nandi Siegfried is Chief Specialist Scientist, Alcohol, Tobacco and Other Drug Research Unit, South African Medical Research Council; Honorary Associate Professor, Department of Mental Health and Psychiatry, Faculty of Health Sciences, University of Cape Town. Charles Parry is Director, Alcohol, Tobacco and Other Drug Research Unit, South African Medical Research Council; Extraordinary Professor, Department of Psychiatry Stellenbosch University.
Acknowledgements: We thank Dr Virginia Zweigenthal for comments, the Western Cape Department of Health for sharing trauma statistics with us and Dr Douglas Parry for data assistance.
Original article available on Maverick Citizen