|
Nada Abdelatif
|
Biostatistics Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Naeemah Abrahams
|
Gender Research Unit, South African Medical Research Council, Cape Town, South Africa and School of Public Health and Family Medicine, University of Cape Town, South Africa.
|
|
Lillian Artz
|
Gender, Health and Justice Research Unit, University of Cape Town, Cape Town, South Africa and Department of Pathology, Division of Forensic Medicine, University of Cape Town, South Africa.
|
|
Oluwatoyin F. Awotiwon
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Olalekan Ayo-Yusuf
|
Research and Graduate Studies, Sefako Makgatho Health Sciences University, Pretoria, South Africa
|
|
Joel Botai
|
Department of Research and Innovation, South African Weather Service, Pretoria, South Africa.
|
|
Debbie Bradshaw
|
Burden of Disease Research Unit, South African Medical Research Council and Division of Epidemiology and Biostatistics, School of Public Health and Family Medicine, University of Cape Town, South Africa.
|
|
Eugene Cairncross
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Kamaseelan Chetty
|
Department of SAAQIS, South African Weather Service, Centurion, South Africa.
|
|
Annibale Cois
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa and Division of Health Systems and Public Health, Department of Global Health, University of Stellenbosch, South Africa.
|
|
Muhammad A. Dhansay
|
Burden of Disease Research Unit, South African Medical Research Council and Division of Human Nutrition, Department of Global Health and Department of Paediatrics and Child Health, Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa.
|
|
Pam Groenewald
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Charl Janse van Rensburg
|
Biostatistics Research Unit, South African Medical Research Council, Pretoria, South Africa.
|
|
Rachel Jewkes
|
Gender and Health Research Unit and Office of the Executive Scientist, South African Medical Research Council, Pretoria, South Africa and School of Public Health, University of the Witwatersrand, Johannesburg, South Africa.
|
|
Jané D. Joubert
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Thandi Kapwata
|
Environment and Health Research Unit, South African Medical Research Council, Pretoria, South Africa.
|
| Reshma Kassanjee |
Centre for Infectious Disease Epidemiology and Research, University of Cape Town, South Africa.
|
|
Andre P. Kenge
|
Non-communicable Diseases Research Unit, South African Medical Research Council, Cape Town, South Africa and Department of Medicine, University of Cape Town, Cape Town, South Africa.
|
|
Demetre Labadarios
|
Professor Emeritus: Faculty of Medicine and Health Sciences, Stellenbosch University, Stellenbosch and Professor Extraordinaire: University of Limpopo.
|
|
Estelle V. Lambert
|
Research Centre for Health through Physical Activity, Lifestyle and Sport, Division of Exercise Science and Sports Medicine, Department of Human Biology, Faculty of Health Sciences, University of Cape Town, South Africa.
|
|
Ria Laubscher
|
Biostatistics Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Naomi Levitt
|
Chronic Disease Initiative for Africa, Department of Medicine, University of Cape Town, Cape Town, South Africa.
|
|
Mercilene Machisa
|
Gender and Health Research Unit, South African Medical Research Council, Pretoria, South Africa and School of Public Health, University of the Witwatersrand, Johannesburg, South Africa.
|
|
Samuel Manda
|
Biostatistics Research Unit, South African Medical Research Council, Pretoria, South Africa and Statistics Department, University of Pretoria, Pretoria, South Africa.
|
|
Richard Matzopoulos
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa and School of Public Health and Family Medicine, University of Cape Town, South Africa.
|
|
Nadine Nannan
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Ian Neethling
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa and Institute for Lifecourse Development, University of Greenwich, Greenwich, London, United Kingdom.
|
|
Johanna H. Nel
|
Department of Logistics, Stellenbosch University, Stellenbosch, South Africa.
|
|
Beatrice Nojilana
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Rosana Pacella
|
Institute for Lifecourse Development, University of Greenwich, Greenwich, London, United Kingdom.
|
|
Charles D.H. Parry
|
Alcohol, Tobacco & Other Drug Research Unit, South African Medical Research Council, Cape Town, South Africa and Department of Psychiatry, Stellenbosch University, Cape Town, South Africa.
|
|
Nasheeta Peer
|
Non-communicable Diseases Research Unit, South African Medical Research Council, Durban, South Africa and Department of Medicine, University of Cape Town, Cape Town, South Africa.
|
|
Victoria Pillay-van Wyk
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Megan Prinsloo
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa and Institute for Lifecourse Development, University of Greenwich, London, United Kingdom.
|
|
Charlotte Probst
|
Institute for Mental Health Policy Research, Centre for Addiction and Mental Health (CAMH), Toronto, Canada and Heidelberg Institute of Global Health (HIGH), Medical Faculty and University Hospital, Heidelberg University, Heidelberg, Germany.
|
|
Rifqah A. Roomaney
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Aletta E. Schutte
|
School of Population Health, University of New South Wales, Australia, The George Institute for Global Health, Sydney, Australia Hypertension in Africa Research Team and South African Medical Research Council Unit for Hypertension and Cardiovascular Disease, North-West University, Potchefstroom, South Africa.
|
|
Freddy Sitas
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa; Centre for Primary Health Care and Equity, School of Population Health, University of NSW-Sydney and Menzies Centre for Health Policy, School of Public Health, University of Sydney.
|
|
Katherine Sorsdahl
|
Alan J Flisher Centre for Public Mental Health, Department of Psychiatry, University of Cape Town, Cape Town, South Africa.
|
|
Nelia P. Steyn
|
Department of Human Biology, Faculty of Health Sciences, University of Cape Town, South Africa.
|
|
Melaku Tesfaye
|
Department of Research and Innovation, South African Weather Service, Centurion, South Africa.
|
|
Eunice B. Turawa
|
Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Lize van Stuijvenberg
|
Non-communicable Disease Research Unit, South African Medical Research Council, Cape Town, South Africa.
|
|
Nicole Vellios
|
Research Unit on the Economics of Excisable Products, University of Cape Town, Cape Town, South Africa.
|
|
Catherine L. Ward
|
Department of Psychology, University of Cape Town, South Africa and Safety and Violence Initiative, University of Cape Town, South Africa.
|
|
Edelweiss Wentzel-Viljoen
|
Centre of Excellence for Nutrition, North-West University, Potchefstroom, South Africa.
|
|
Caradee Y. Wright
|
Environment and Health Research Unit, South African Medical Research Council, Pretoria, South Africa and Department of Geography, Geoinformatics and Meteorology, University of Pretoria, Pretoria, South Africa.
|
|
|
Trend in attributable burden of each risk factor
|
What does it mean?
|
|
|
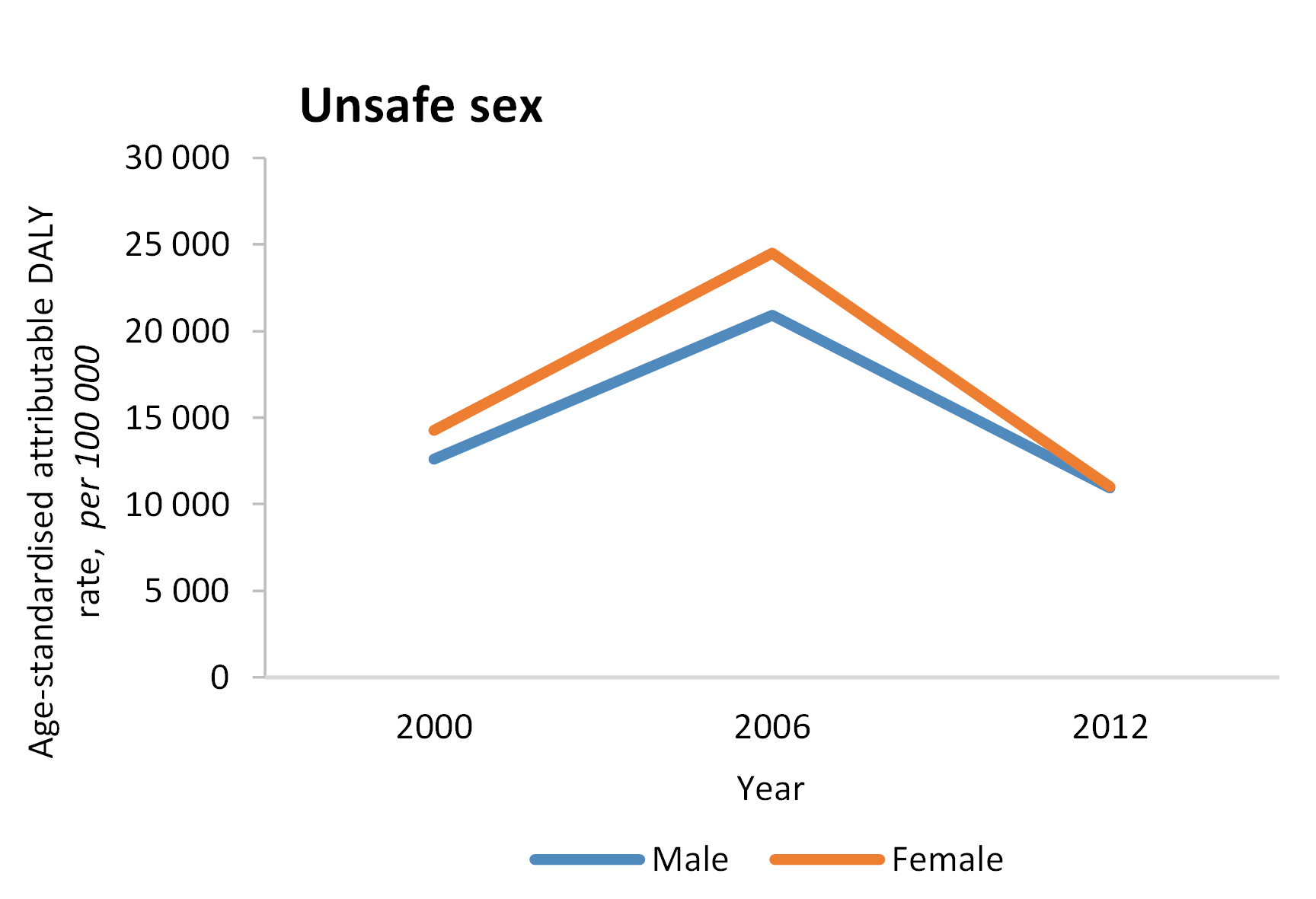
- The year 2006 represented the peak of the HIV epidemic and there has been a significant decline in the DALYs attributable to HIV by 2012
- This is still the leading cause of DALY so intensive programming is still required for South Africa to meet international goals in HIV reduction and management e.g., medical male circumcision campaigns, and risk awareness campaigns.
- HPV vaccination coverage for young girls must be extended to maximise the potential for preventing cervical cancer.
|
|
|
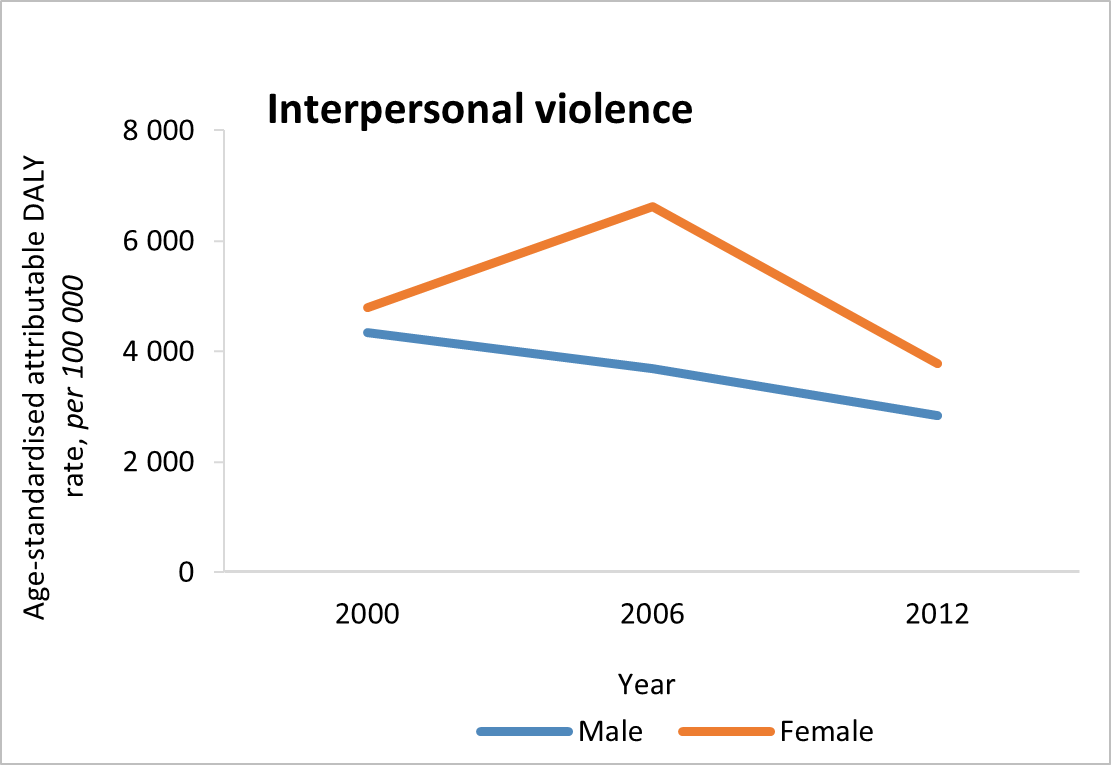
- Rates of interpersonal violence have decreased for men but remain unchanged for women in the period 2000 to 2012.
- Despite a decline in interpersonal violence, the exceedingly high burden indicates that South Africa requires further reinforcement and strengthening of the implementation of existing laws on and responses to gender-based violence, child protection and firearm use, and other prevention programmes to address the burden of violence.
|
|
|
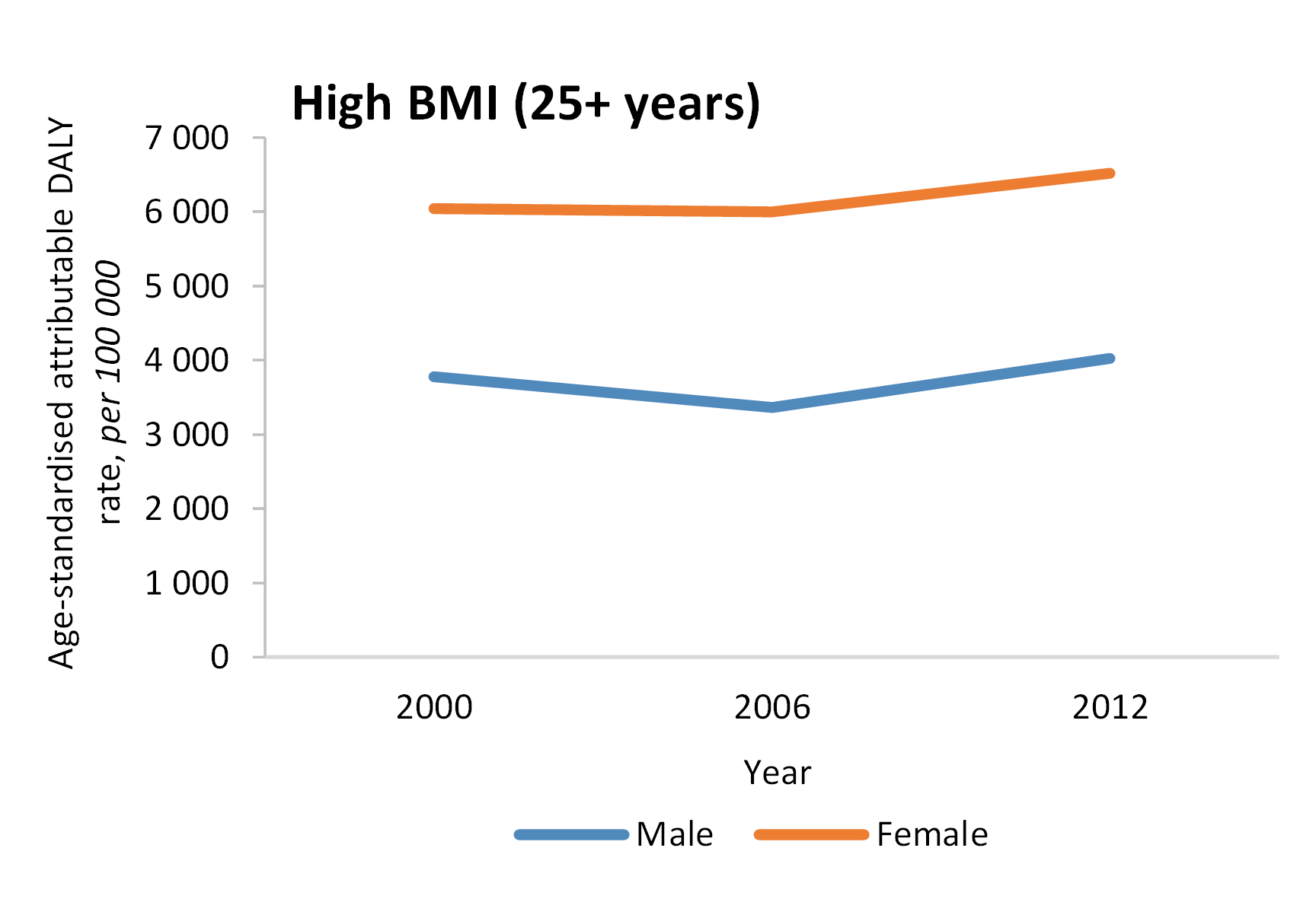
- The average BMI increased between 2000 and 2012, with DALY rates also increasing.
- Although obesity prevention strategies have been initiated by the Department of Health, a comprehensive framework is needed to target underlying determinants such as food systems, urban systems, and economic systems to stem the increasing prevalence of obesity.
|
|
|
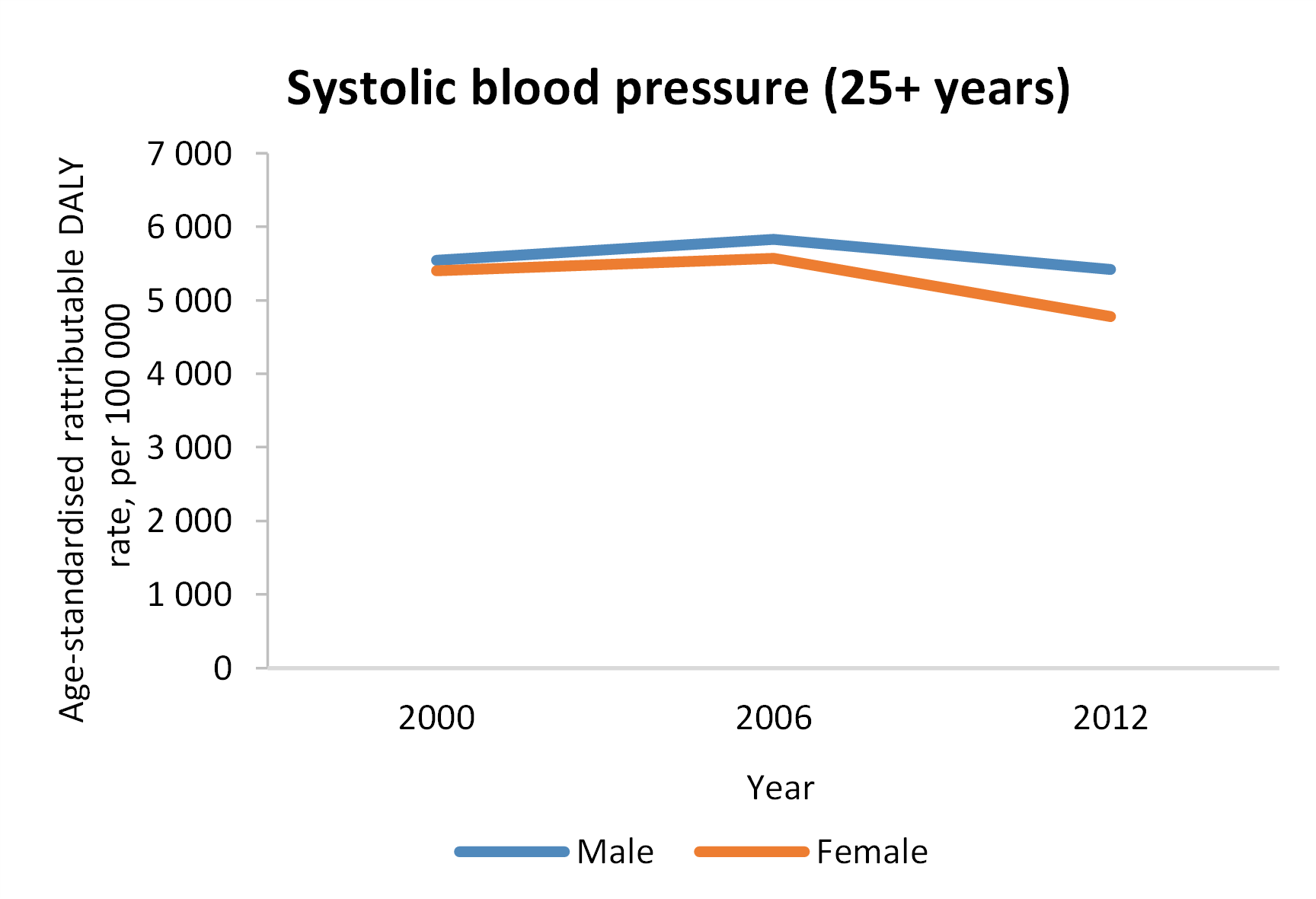
- DALYs related to systolic blood pressure have decreased since 2006, however, this could be related to an increase in treatment for hypertension.
- More preventative strategies are needed, accompanied by improved diagnosis and care of hypertension.
|
|
|
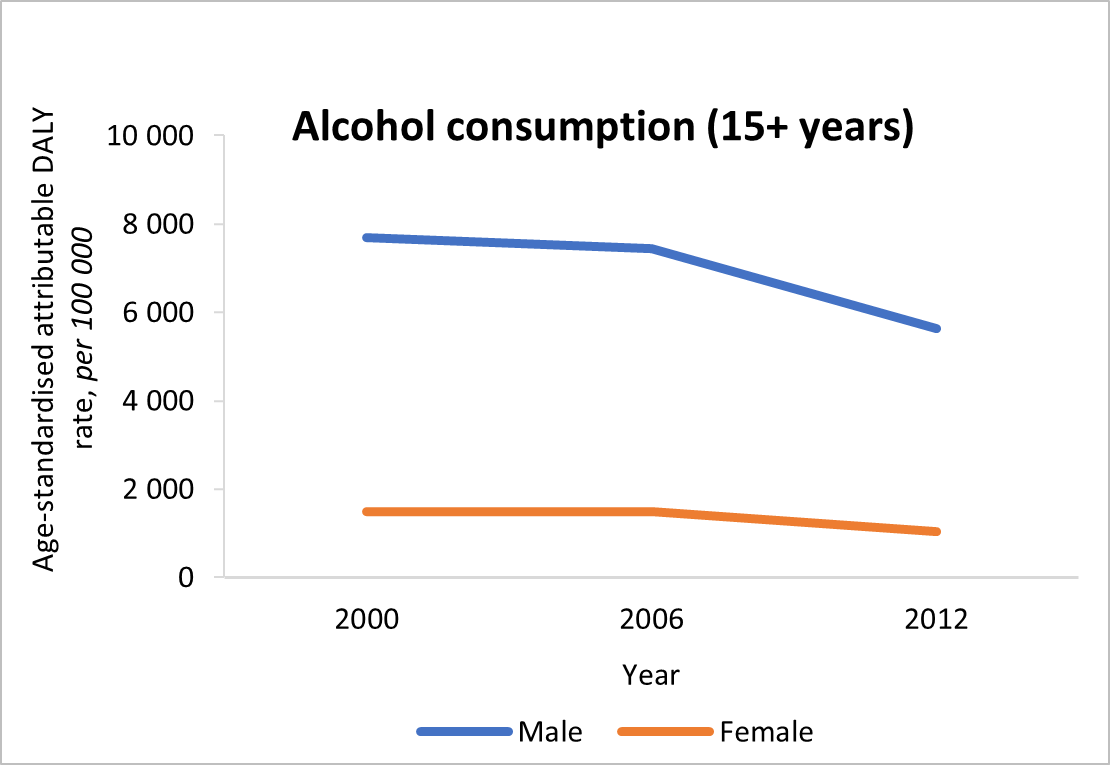
- DALYs due to alcohol consumption have decreased in men but increased in women.
- Despite previous recommendations for interventions, the burden due to alcohol remains large and much more vigorous implementation of existing measures is required to address the harm due to alcohol.
|
|
|
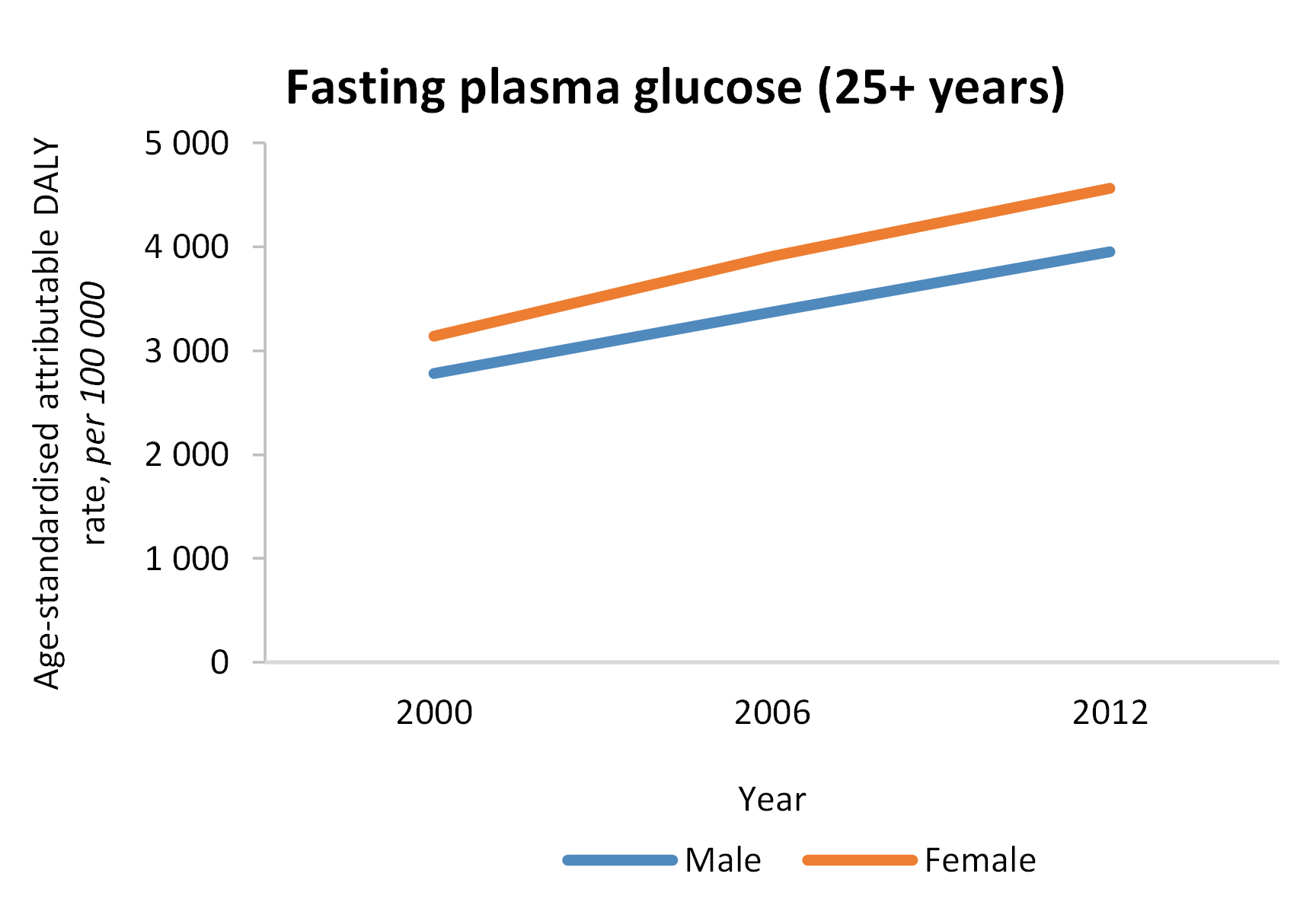
- There has been a concerning increase in the DALY rate attributable to fasting plasma glucose.
- A multi-pronged approach is required to reduce the burden, including, mass screening and promotion of the uptake of healthy activities. Diagnosis, treatment and control also need to be promoted.
|
|
|
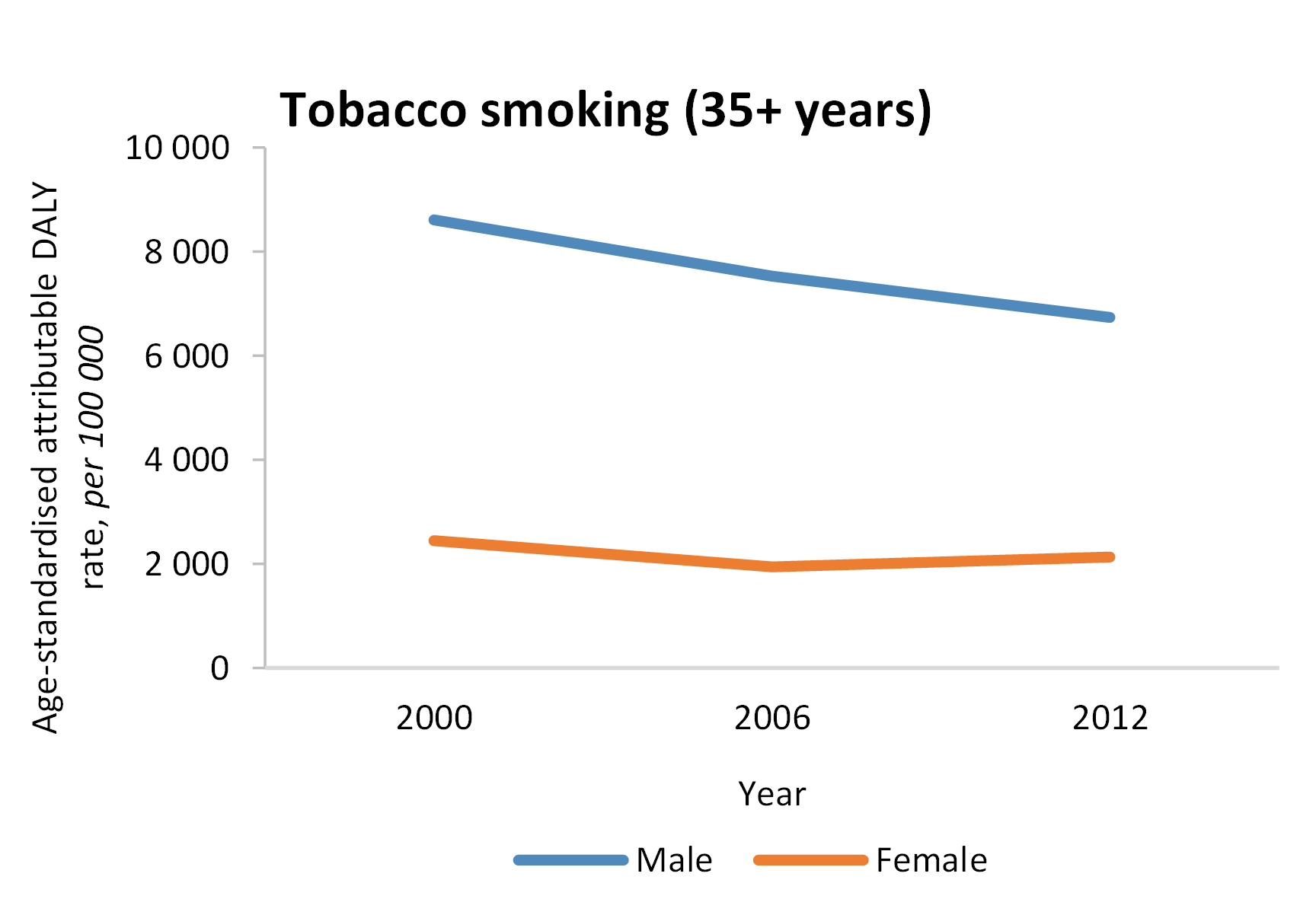
- Rates of decline in smoking prevalence have plateaued between 2010 and 2012, suggesting that tobacco control measures need review and strengthening
- Increasing excise taxes is the most effective measure to reduce smoking prevalence and should be implemented along with a track and trace system to improve tax compliance and reduce illicit trade. In-clinic interventions for high-risk patients are also required for intensive cessation support.
|
|
|
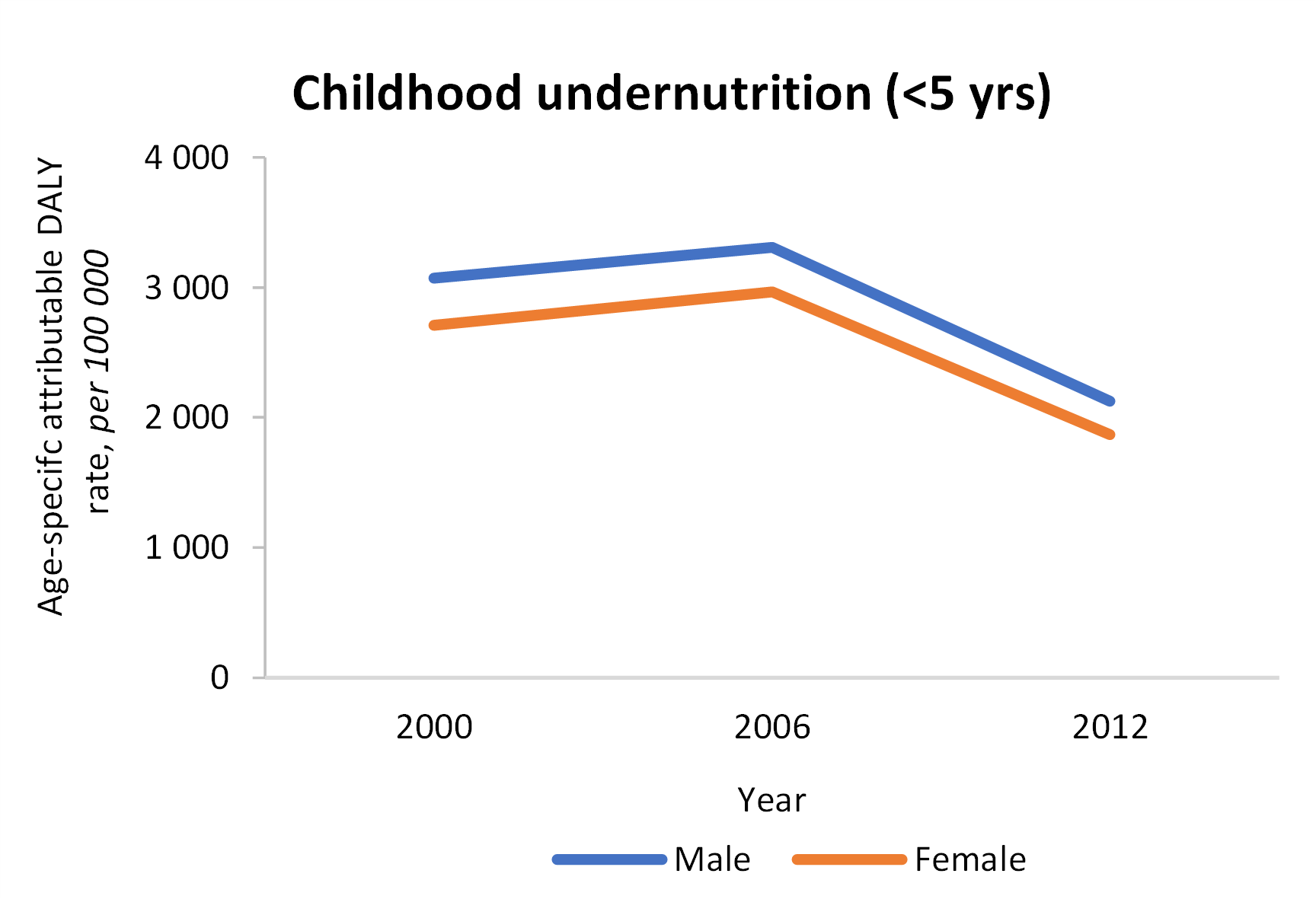
- Despite a reduction since 2006, an estimated 33% of child deaths in South Africa were attributable to undernutrition.
- Addressing undernutrition must include measures that address household poverty and food security, and ensuring nutrition as a basic human right. The health system response also needs to be strengthened. Also, regarding, routine child nutrition surveillance, current programs need to be evaluated.
|
|
|
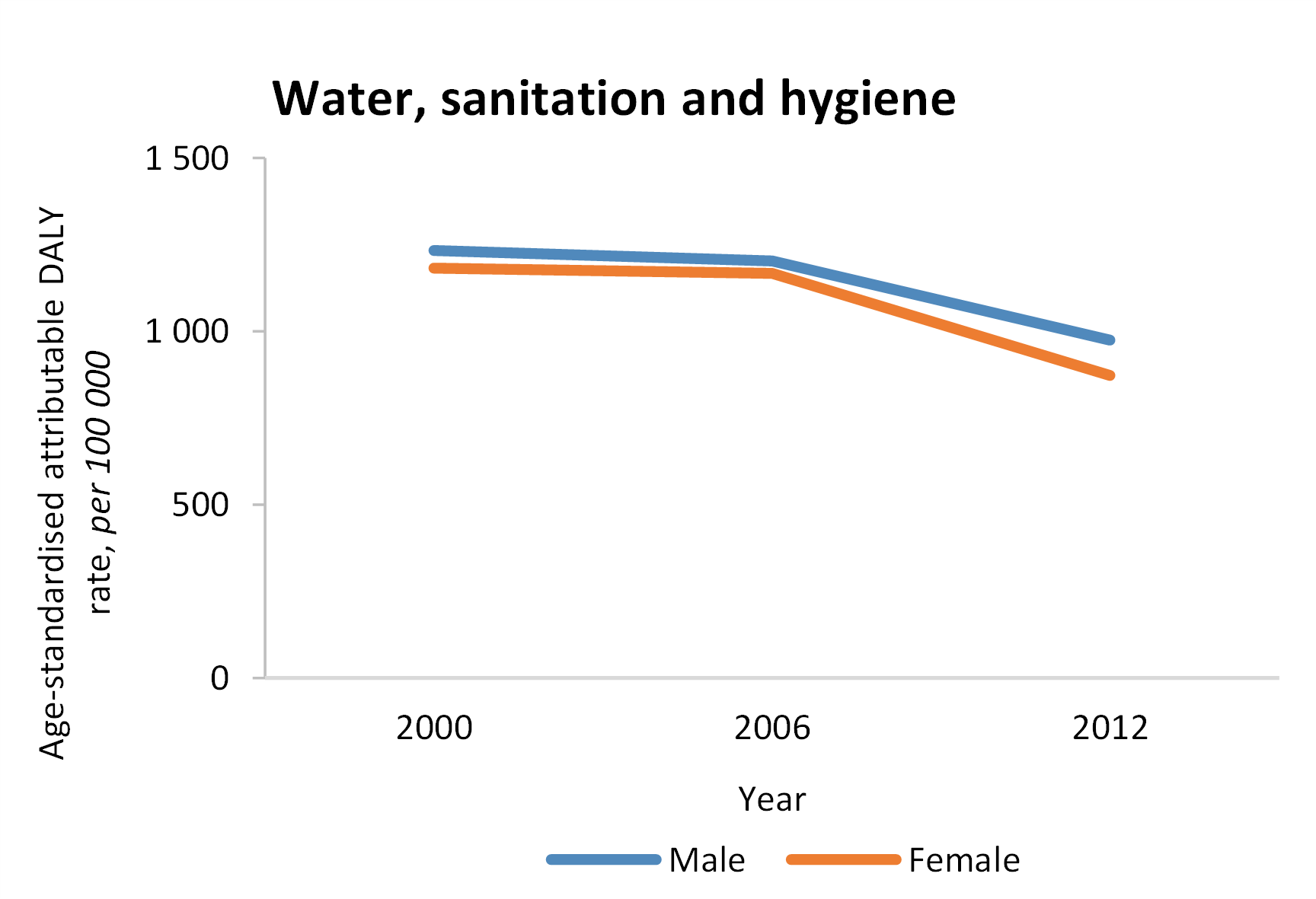
- There has been a slight reduction in DALYs due to water, sanitation, and hygiene since 2006. However, there are stark provincial inequalities in attributable burden, mediated through good versus poor water and sanitation supply and unequal improvement in water and sanitation supply across provinces.
- High priority needs to be given to improving access to safe and sustainable sanitation and water supply, particularly in underserved urban and rural communities in South Africa.
|
|
|
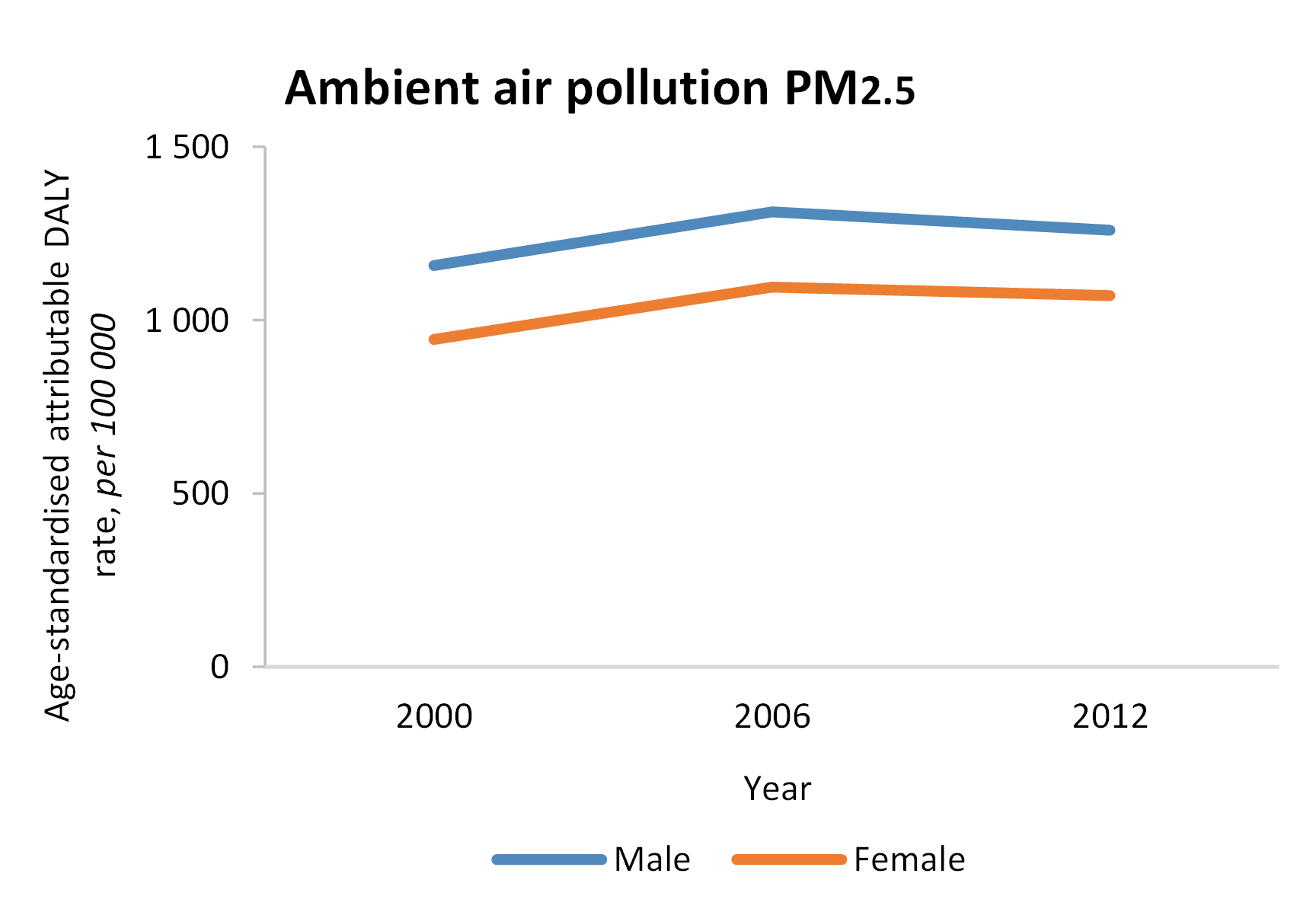
- The vast majority of South Africans were exposed to harmful levels of ambient air pollution in the period.
- Efforts are needed to reduce ambient air pollution in the country by enforcing national air quality standards and lowering the reliance on fossil fuels.
|
|
|
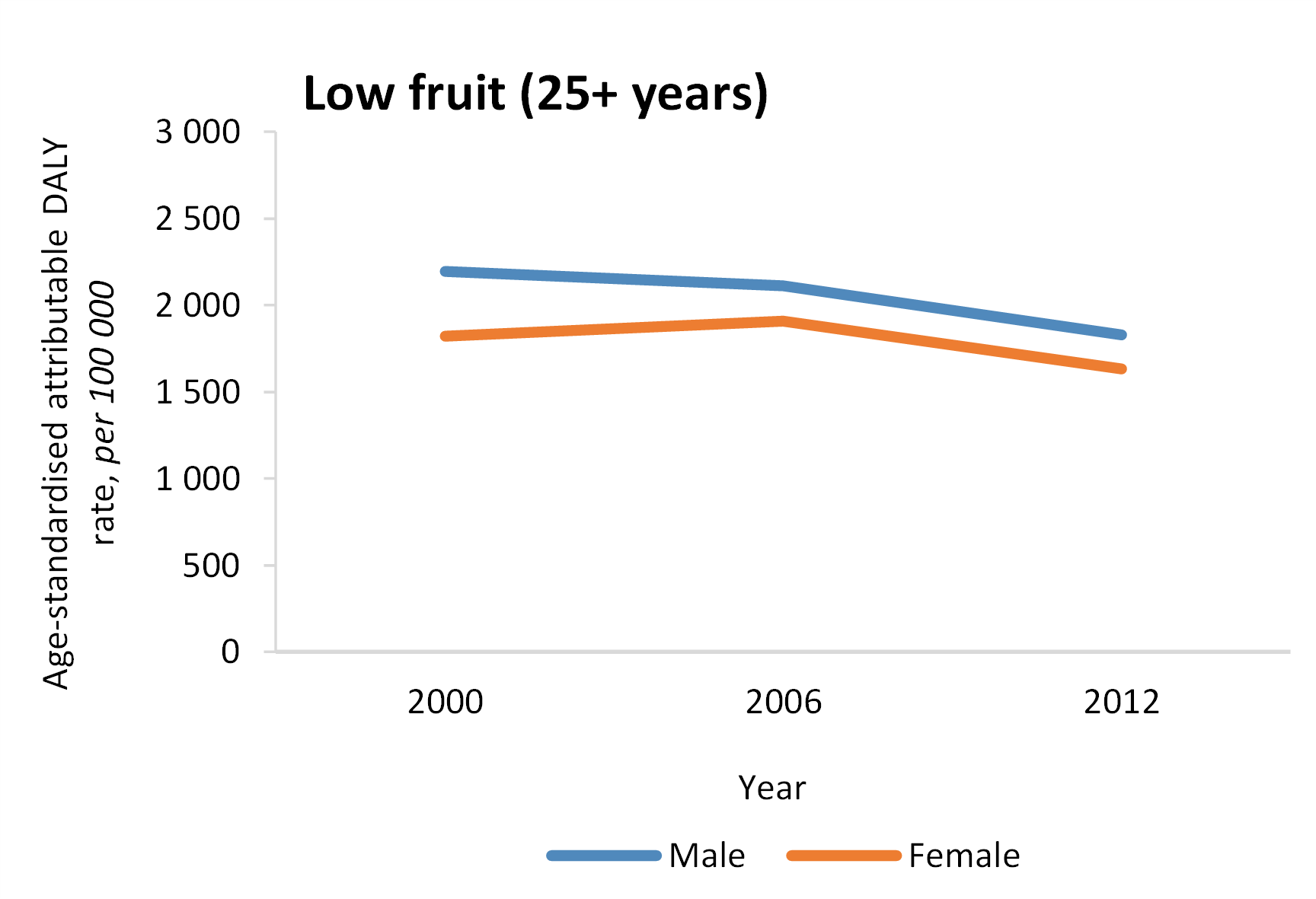
- The average intake of fruit decreased between 2000 and 2012, and the DALY burden decreased.
- The burden of disease attributable to a diet low in fruits remains high and effective interventions supported by legislation and policy are needed to reverse the declining trends in fruit consumption observed across most age groups.
|
|
|
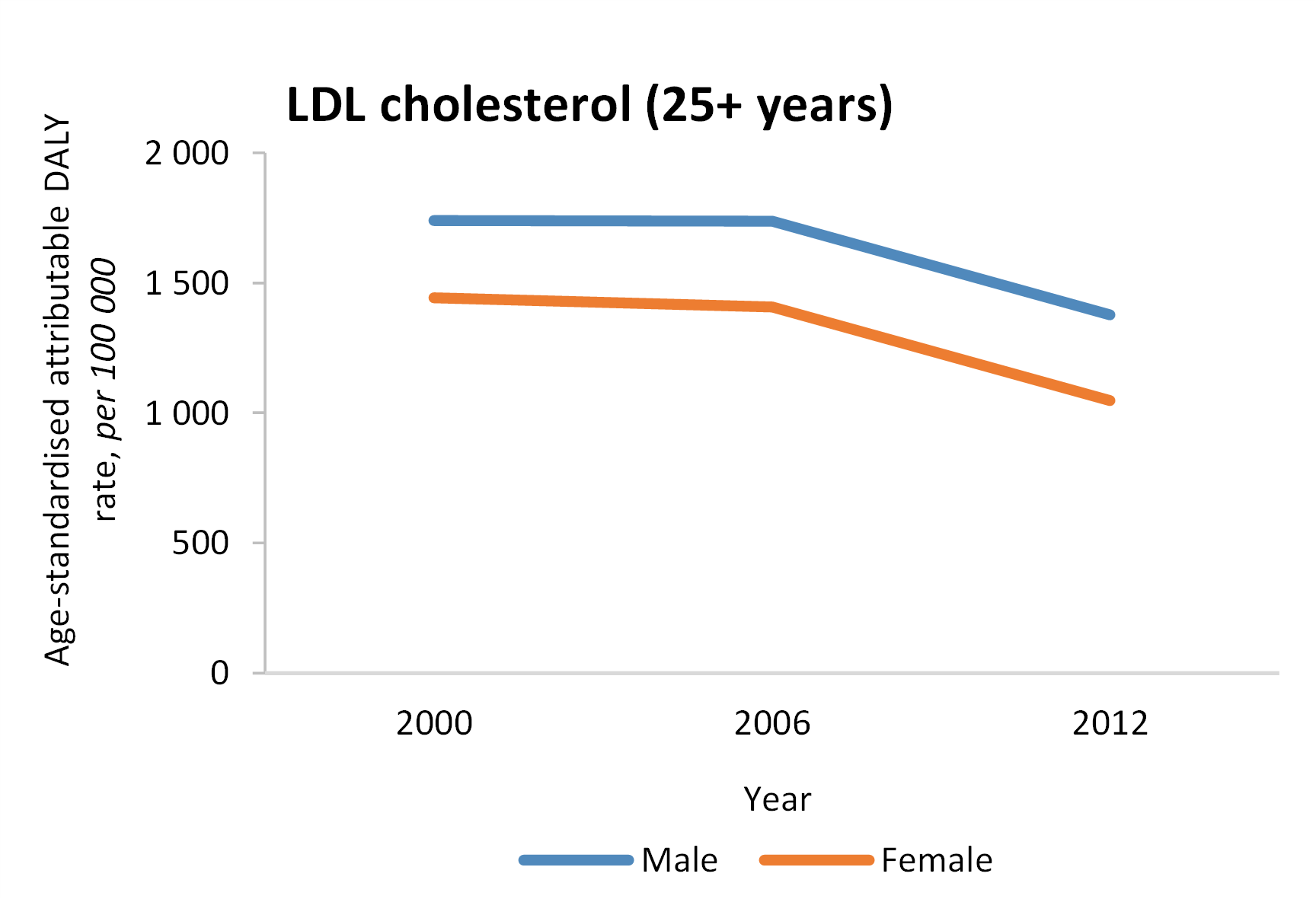
- The burden due to LDL cholesterol decreased between 2000 and 2012.
- Mean population LDL cholesterol values remain high and can be lowered further through nationwide nutrition education programmes, collaboration with the food industry to improve labelling and cheaper pricing of healthy foods.
|
|
|
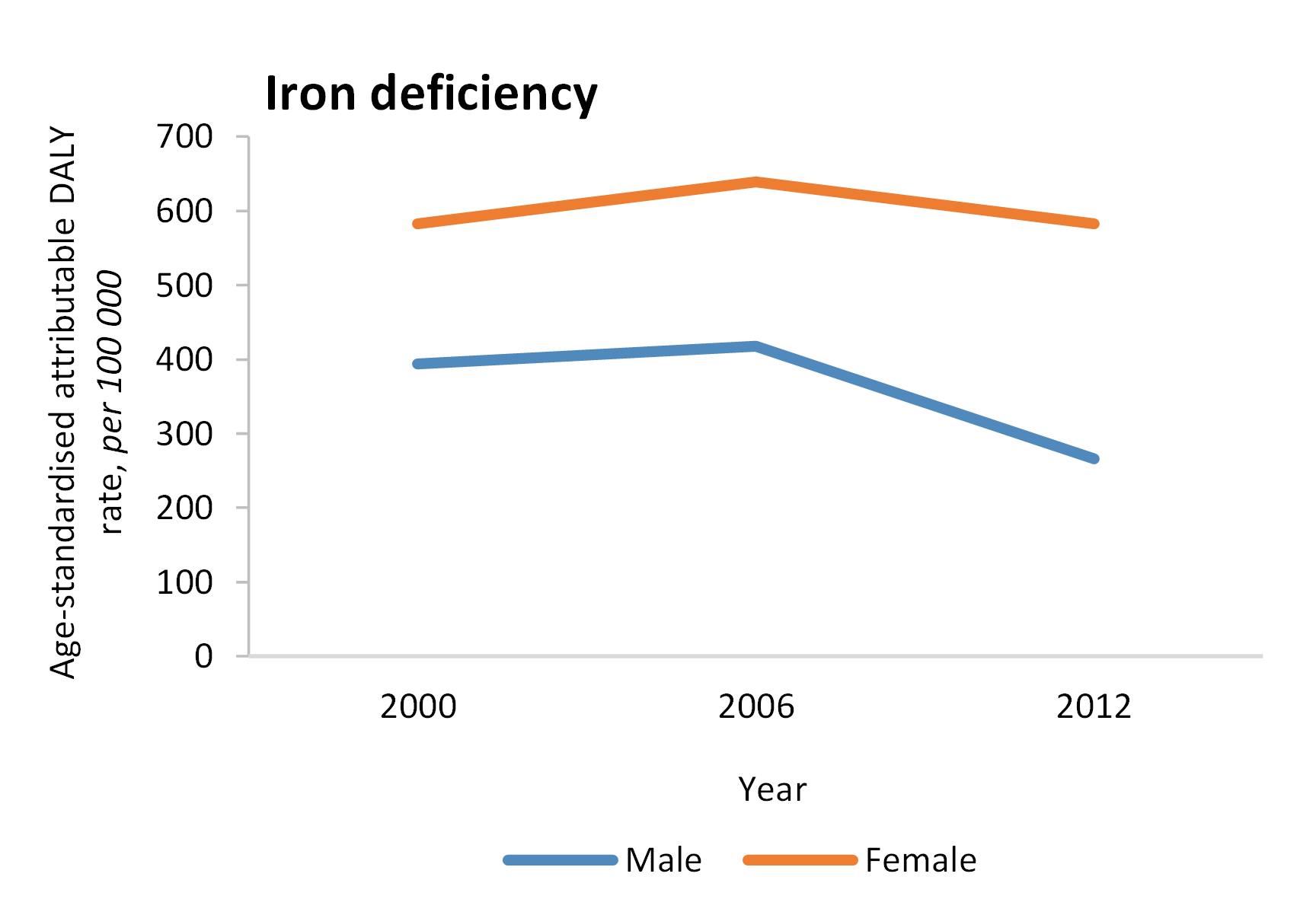
- There has been a decrease in the DALY rate attributable to iron deficiency.
- However, iron-deficiency anaemia prevalence can be markedly reduced if iron deficiency is eliminated. Hence, it is essential to encourage, measures that have been implemented to address iron deficiency, including food fortification and the iron supplementation programme for infants over 6 months of age and women of reproductive age.
- The intersection of anaemia and HIV especially amongst pregnant women, requires that the dietary requirement of these individuals be evaluated.
|
|
|
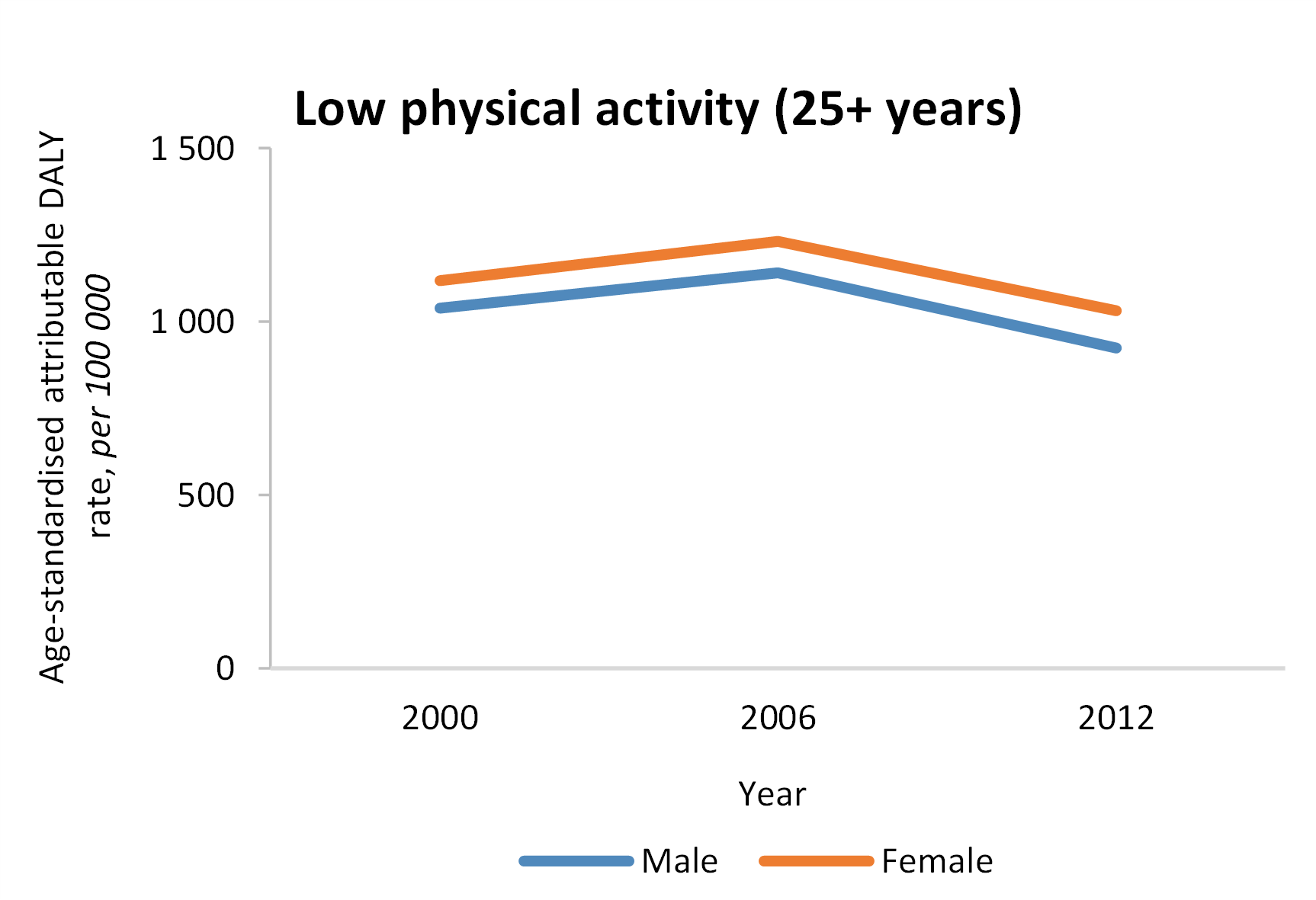
- DALY rates due to low physical activity decreased between 2000 and 2006.
- The burden still remains high, indicating that existing policies need to be implemented so that there is universal access to sports and recreational facilities, as well as walkable communities.
|
|
|
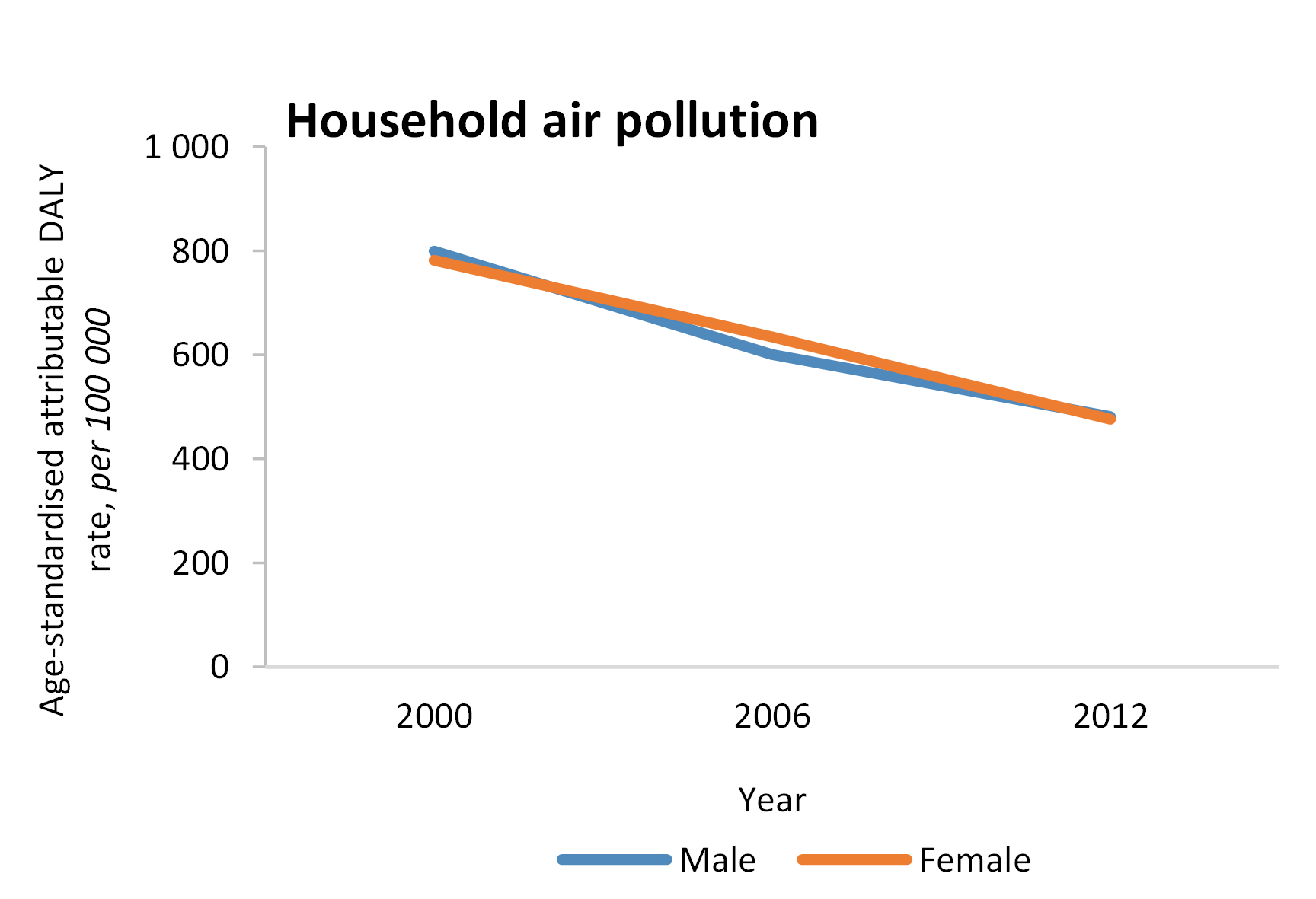
- The DALY rate attributable to household air pollution due to cooking with solid fuels has reduced between 2000 and 2012.
- Legislation and interventions are needed to eradicate the use of solid fuels, especially in the light of worsened loadshedding in the country.
|
|
|
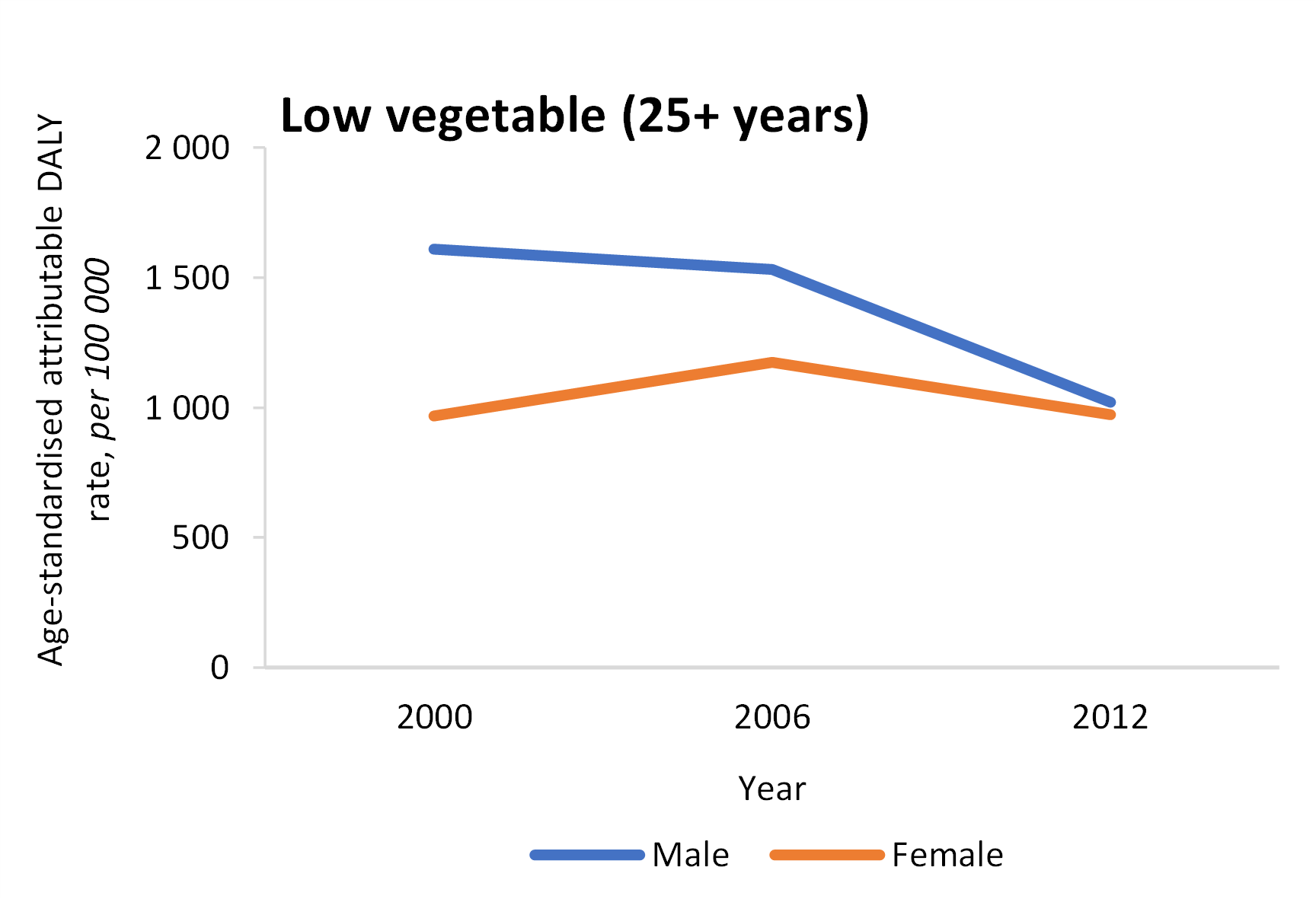
- The average intake of vegetables decreased between 2000 and 2012.
- The burden of disease attributable to a diet low in vegetables remain high and effective interventions are needed to increase vegetable consumption.
|
|
|
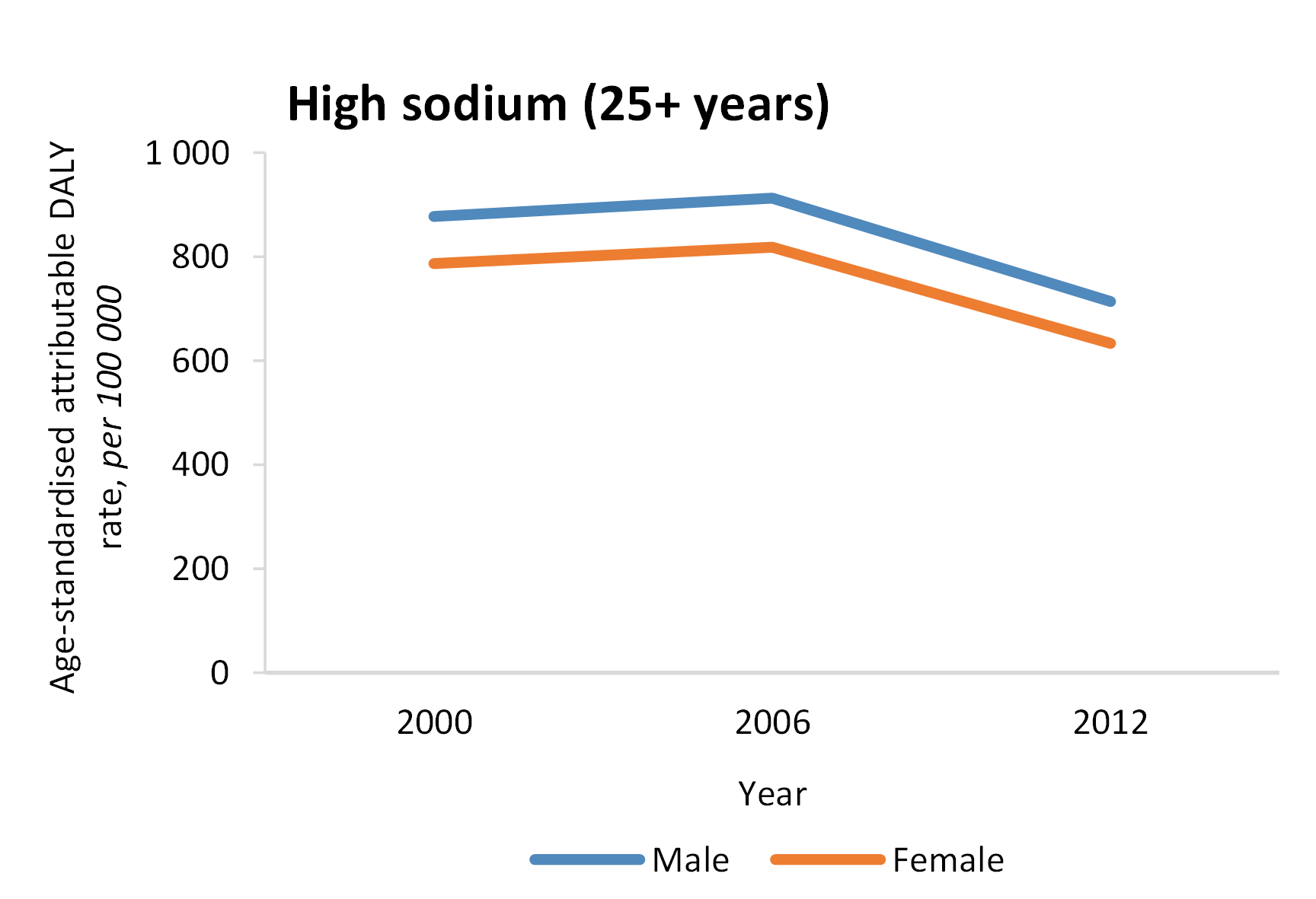
- There has been a decrease in the DALY rate due to high sodium between 2000 and 2012.
- The regulation of salt content is a step in the right direction, but sustained effort is needed to also monitor sodium consumption to reduce the risk of cardiovascular disease.
|
|
|
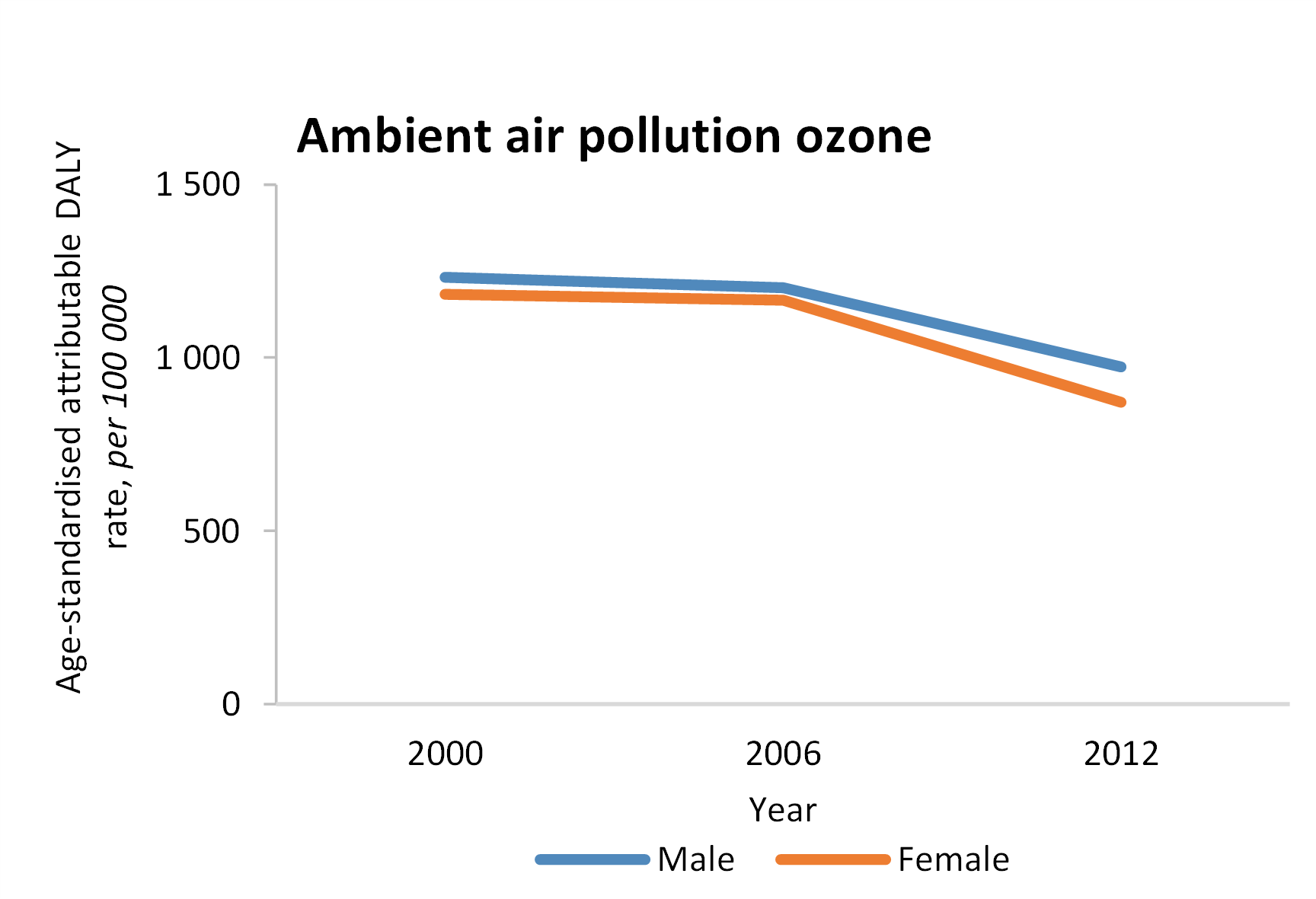
- There has been a drop in age-standardised DALYs between 2000 and 2006.
- National air quality standards for ozone need to be enforced.
|
|